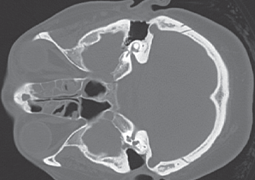
Orbital complications of sinusitis in the sense of Chandler’s classification represent an emergency condition, requiring quick diagnosis and aggressive treatment. Rhinoendoscopy, ophthalmological examination and CT of the paranasal sinuses and orbit enable determination of the stage and origin of the complications. In the case of periorbital cellulitis and the early stage of orbital cellulitis, conservative intravenous antibiotic therapy is possible. Monitoring of the inflammation parameters and the ocular finding is mandatory. In the case of lack of improvement or deterioration of the symptoms within 24-48 hours and in more advanced stages of orbital complications, surgical treatment is also essential. The aim of the study was to evaluate orbital complications of inflammation of the paranasal sinuses with regard to epidemiology, clinical symptoms and management. Retrospective data was evaluated from 8 patients who were admitted to the Department of ORL and Head and Neck Surgery of the Louis Pasteur Teaching Hospital in Košice with suspected sinogenic orbital complications from 2008 to 2013. The patients were analysed in terms of gender, age, CT findings, microbiology, clinical symptoms, stage of complication and treatment. Males and females were afflicted within a ratio of 1.66:1. Young adults in their 20s and 30s predominated (62.5%). Acute and chronic sinusitis were the cause of orbital complications in equal proportions. The most common origin of complications was ethmoid sinusitis (62.5%), followed by maxillary (25%) and frontal (12.5%) sinusitis. An image of polysinusitis with affliction of the ethmoid, maxillary and frontal sinuses (75%) predominated on CT of the paranasal sinuses. Staphylococcus epidermidis and Staphylococcus aureus were determined as the etiological agents in half the cases. The ocular symptoms recorded were: periorbital edema (100%) protrusion of the eyeball, restriction of movement, chemosis of the conjunctiva (50%), diplopia and secondary glaucoma (12.5%). On the basis of the conducted examinations, preseptal cellulitis – stage I was diagnosed in 3 cases (37.5%), orbital cellulitis – stage II in 3 cases (37.5%) and subperiosteal abscess – stage III in 2 cases (25%). Combined therapy was applied to all the patients (100%) – i.v. antibiotics and surgical treatment within 24 hours. Eradication of the disease from the area of the ostiomeatal complex (OMC), drainage of the afflicted sinuses and drainage of the subperiosteal abscess were performed by the method of functional endonasal endoscopic surgery (FEES). In the case of a superior subperiosteal abscess, a combined endonasal and external approach (external orbitotomy) was required. The average period of hospitalisation was 7 days. Quick diagnosis and aggressive combined therapy of orbital complications of inflammation of sinusitis reduces the danger of prevent loss of vision and life-threatening complications.
- Actual State of the One Day Simultaneous Bilateral Cataract Surgery Issue
- The Effectiveness of Corneal Cross-Linking in Stopping the Progression of Keratoconus
- Corneal Transplantations in the Czech Republic in 2012
- The Molecular Genetic Cause and Clinical Findings in two Probands with Stargardt Disease
- Orbital Complications of Sinusitis
- Mobile Telephones as Devices for Documentation of the Ocular Fundus